















 35 148
35 148

3.
Results
Table 1summarizes the clinicopathologic characteristics of
the study cohort from which patient-reported data were
obtained. Median patient age in this cohort was 62
(interquartile range: 57- 67) yr, with a median reported
baseline IIEF-6 score of 28 (interquartile range: 21
–
30).
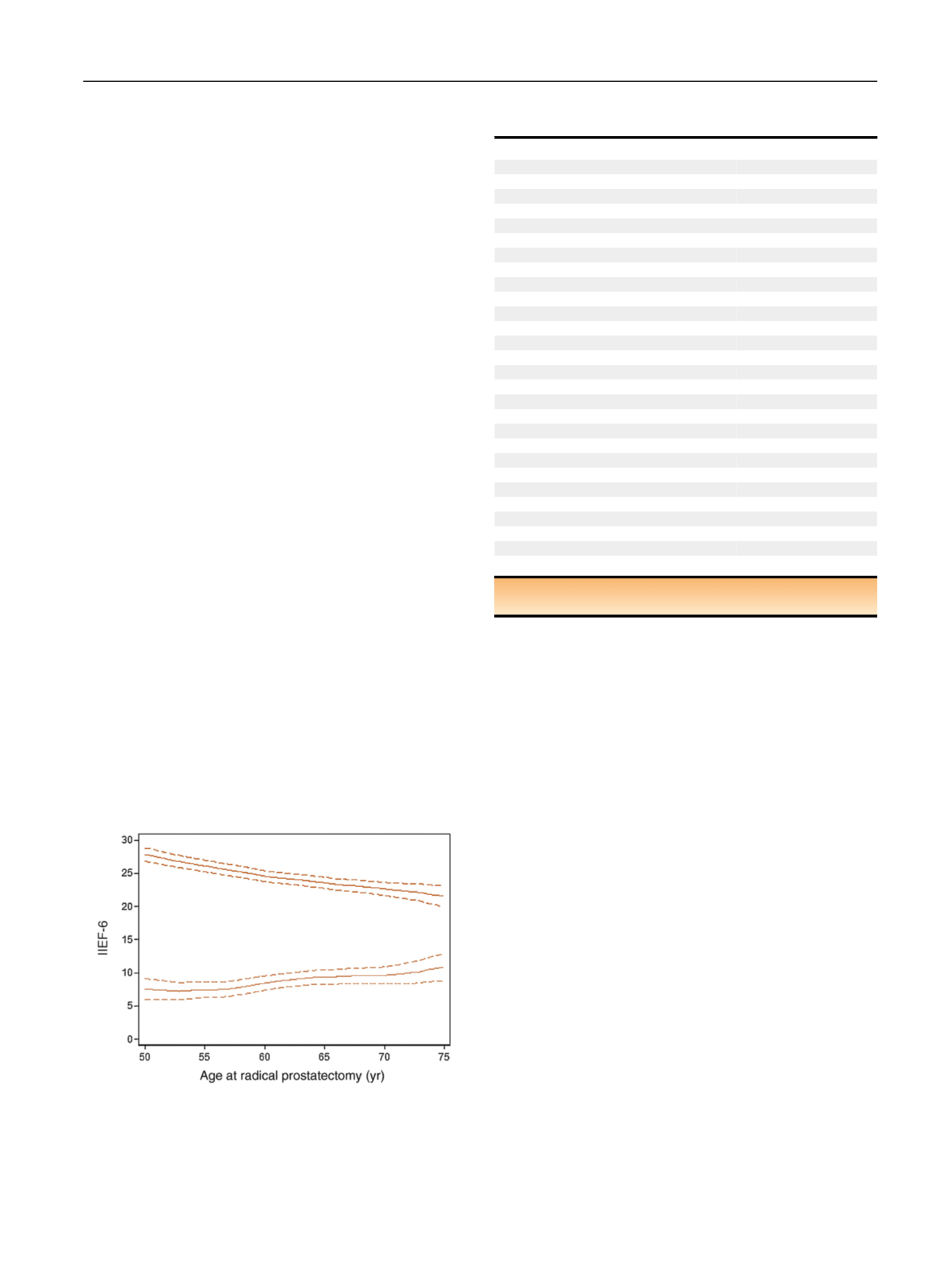
Each year increase in patient age resulted in a
[10_TD$DIFF]
0.27 (95%
CI:
[16_TD$DIFF]
0.18,
[17_TD$DIFF]
0.36,
p
<
0.0001) point reduction in baseline IIEF
scores
( Fig. 1). Comorbidity reduced baseline scores, with a
[18_TD
$DIFF]
0.81 (95% CI
[19_TD$DIFF]
2.01,
[20_TD$DIFF]
0.38;
p
=
[21_TD$DIFF]
0.2),
[22_TD$DIFF]
3.02 (95% CI
[23_TD$DIFF]
4.40,
[24_TD$DIFF]
1.65;
p
<
0.0001), and
[25_TD$DIFF]
3.77 (95% CI
[26_TD$DIFF]
5.58,
[27_TD$DIFF]
1.96;
p
<
0.0001) point change in IIEF for one, two, or three or
more comorbidities. However, there was no evidence that
erectile function declined faster with increasing age in
patients with comorbidities (
p
=
[28_TD$DIFF]
0.16 for the interaction
term). As such, comorbidities were excluded from the
model estimating postoperative recovery.
The degree of erectile function recovery after RP also
decreases (
[11_TD$DIFF]
0.16
[12_TD$DIFF]
IIF points/yr, 95% CI
[13_TD$DIFF]
0.27,
[14_TD$DIFF]
0.05,
p
=
[15_TD$DIFF]
0.006). For example, a typical 55-yr-old patient would lose
7.5 points from pre-RP to 12-mo post-RP; a 60-yr-old
patient who would lose 8.4 points
( Fig. 1 ).
Fig. 2illustrates the predicted erectile function scores
over time for a 55-yr-old patient with a baseline IIEF-6 score
of 26 with immediate versus surgery delayed by 5 yr, a
timepoint at which about a third of men initially managed
on active surveillance have been treated
[2] .The average 10-
yr IIEF score was higher on delayed surgery (2.1 points, 95%
CI: 0.4, 3.9). Indeed, even if we assume a very short delay to
surgery of only 3 yr, we continue to see a significant
improvement compared with immediate treatment
(1.5 points, 95% CI: 0.2, 3.0).
We repeated these analyses for men aged 60 yr and 65 yr
looking over 10-yr and 15-yr timeframes with similar
results
( Table 2). For example, a man diagnosed with
prostate cancer at 65 yr old would have an average of
3.3 more points on the IIEF-6 over a 10-yr period if RP were
delayed for 5 yr (95% CI: 1.8, 4.6). In each scenario, delayed
RP was estimated to lead to an increase inmean IIEF-6 score,
although differences between groups were not statistically
significant in all cases.
As erectile function was superior on active surveillance
even if a man was subject to surgery after a relatively short
duration, incorporation of longer delays to surgery, or no
surgery at all, would have no effect on our conclusion that
erectile function is superior on delayed surgery. According-
ly, these planned analyses were not conducted.
4.
Discussion
Using a robust database of baseline and postoperative
patient reported outcomes for men with low- and
intermediate-risk prostate cancer, we found that the
predicted average long-term erectile function is higher
for men who undergo delayed compared with immediate
RP at a younger age. Our findings disconfirm the hypothesis
that early surgery compared with active surveillance
improves sexual function by utilizing a window of
opportunity for postoperative recovery. Indeed, the results
suggest that a man should opt for active surveillance even if
he knew that surgery would be required within a few years.
Our data can be compared with other reports in the
literature. First, there is clear evidence for our finding that
recovery is age-related. Brajtbord et al
[7]report erectile
recovery after RP in two age groups,
60 yr and
>
60 yr.
Older men were more likely to have a
“
clinically significant
”
Table 1
–
Clinicopathologic characteristics of cohort (
n
= 1103; data
are given as median and quartiles or frequency and percentage)
Age (yr)
62 (57, 67)
Preoperative IIEF-6
28 (21, 30)
Preoperative PSA (ng/ml)
4.9 (3.6, 6.5)
Biopsy cores (
N
=
[5_TD$DIFF]
1095)
12 (6, 13)
Positive biopsy cores (
N
=
[6_TD$DIFF]
1099)
3 (1, 5)
Biopsy Gleason grade group
1
566 (51%)
2
537 (49%)
RP Gleason
[7_TD$DIFF]
grade group
1
264 (22%)
2
681 (62%)
3
153 (14%)
4
13 (1.2%)
5
12 (1.1%)
T Stage
pT2c
810 (73%)
pT3a
259 (23%)
pT3b
34 (3.1%)
Positive surgical margins
151 (14%)
Unknown
1 (
<
0.1%)
Comorbidities
0
372 (34%)
1
390 (35%)
2
234 (21%)
3+
107 (10%)
Type of surgery
Laproscopic
288 (26%)
Open
294 (27%)
Robotically-assisted laproscopic
521 (47%)
IIEF-6 = International Index of Erectile Function-6; PSA = prostate-speci
fi
c
antigen.
[(Fig._1)TD$FIG]
Fig. 1
–
Effects of age on erectile function and recovery of erectile
function after radical prostatectomy. Black line
[3_TD$DIFF]
: International Index of
Erectile Function-6 (IIEF-6) measured erectile function by age. Grey line
[4_TD$DIFF]
:
loss in IIEF-6 measured erectile function from pre- to 12-mo postradical
prostatectomy by age. Dashed lines are 95% confidence intervals. Older
patients have lower baseline IIEF scores and experience larger losses in
erectile function compared to younger patients after surgery.
E U R O P E A N U R O L O GY 7 3 ( 2 0 18 ) 3 3
–
3 7
35