















 36 148
36 148

decrease in sexual outcomes, particularly bother. In a paper
describing a prediction model for postoperative erectile
dysfunction
[2_TD$DIFF]
, Alemozaffar et al
[5]reported that increasing
age was associated with a decreased probability of erectile
function, even after adjusting for baseline function. The
time course of erectile function we report can be compared
with data from the Prostate Cancer Outcomes Study
[8] .Results are similar except that erectile function recovery
appears better in the current study, possibly due to the
differences between specialist and community settings.
Poorer recovery overall would push our results even further
in favor of delayed surgery.
Donovan et al
[6]report erectile function over a 6-yr
period in the ProtecT randomized trial comparing surgery
with active surveillance. Men in the surveillance groupwere
subject to treatment on progression
—
with approximately
35% being treated by 6 yr
[9]—
and hence the outcome
reported includes declines associated both with aging and
with treatment. Erectile function was superior in the active
surveillance arm compared with surgery, supporting our
principal findings. The other major randomized trial that
compares surgery with conservative management is SPGC4.
The authors report rates of erectile dysfunction of 66%
versus 24% and 81% versus 75% at 4 yr and 12 yr, respectively
[10] .While this lends general support to our findings, SPCG4
is not directly relevant to current practice as patients in the
conservative management group were not as aggressively
followed as would be typical for contemporary active
surveillance approaches. As such, the rate of treatment was
lower
—
less than 20% at 10 yr
—
leading to lower rates of
treatment-related erectile dysfunction.
The advantage of using a modeling approached based on
empirical data compared with studies, such as ProtecT,
based on empirical data alone, is our ability to model
follow-up over a 10
–
15-yr period. That said, modeling
approaches do have limitations. One major assumption we
make is that cross-sectional data on preoperative function
by age can be used to estimate how erectile function would
change over time on an active surveillance program. As
there is no strong evidence that aspects of active surveil-
lance such as repeat biopsy
[11,12]have a strong effect on
erectile function, age-related declines seem the most
reasonable hypothesis.
Due to limited data on long-term recovery by age, we
assume that recovery is complete by 2 yr, even though there
is evidence that erectile function continues to recover in
some men after this time point
[13]. This type of
underestimation of recovery would constitute a bias against
immediate surgery. However, we do not incorporate
discounting, the principle that having something now is
more valuable than having it later. One recommended rate
of discounting for health outcomes is 1.5
–
2%
[14], equiva-
lent to 14
–
18% over 10 yr. The theory behind immediate
surgery is that although a patient will suffer short-term
morbidity, long-term recovery will be superior. Failure to
incorporate discounting is therefore a bias towards
immediate surgery. Our best guess is that these two
biases
—
longer-term recovery and discounting
—
are approx-
imately equal and so would not have a large effect on our
conclusions.
We also assume that IIEF is linearly associated with
erectile function, that is, a given change in IIEF is equally
important to a man at all levels of IIEF. This is unlikely to be
true as, say, a difference between an IIEF of 5 versus 8 has no
impact on a man
’
s sex life, whereas a difference between
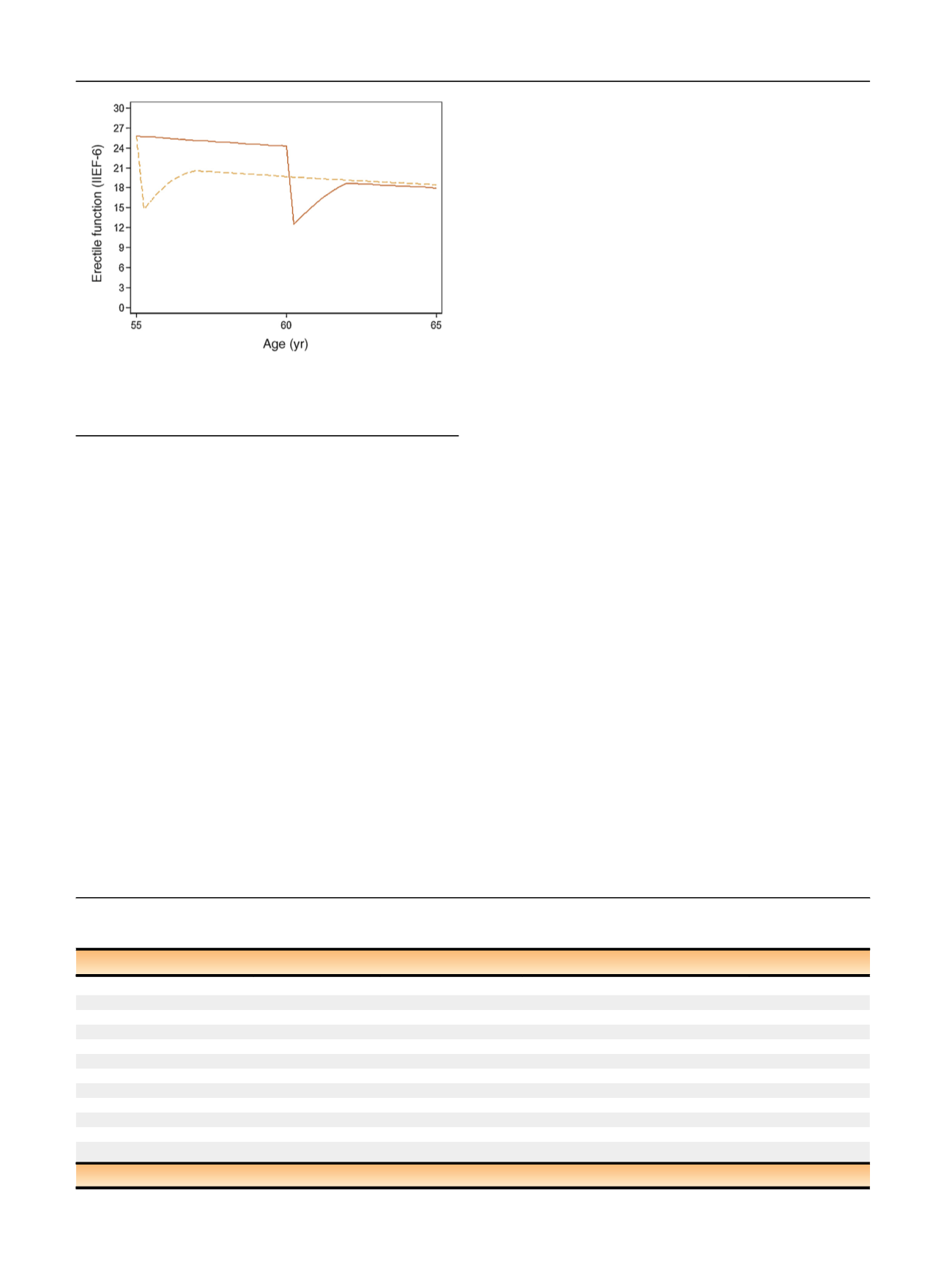
[(Fig._2)TD$FIG]
Fig. 2
–
Erectile function scores over time for a 55-yr-old patient with
a baseline International Index of Erectile Function-6 (IIEF-6) score of
26 with immediate (dashed line) versus surgery delayed by 5 yr
(solid line).
Table 2
–
Difference in mean International Index of Erectile Function-6 (IIEF-6) score over a 10-yr or 15-yr time frame after prostate cancer
diagnosis (comparing immediate radical prostatectomy to 3-yr and 5-yr delays in surgery)
Age at diagnosis (yr)
RP delay (yr)
Time frame (yr)
Difference in mean IIEF-6 score
95% CI for difference
55
3
10
1.5
0.2, 3.0
15
1.0
–
0.2, 2.8
5
10
2.1
0.4, 3.9
15
1.3
–
0.5, 3.3
60
3
10
0.8
–
0.6, 1.8
15
0.2
–
1.3, 1.3
5
10
1.9
0.3, 3.1
15
0.8
–
0.9, 2.1
65
3
10
1.9
0.9, 3.0
15
1.3
0.1, 2.4
5
10
3.3
1.8, 4.6
15
2.2
0.4, 3.6
CI = con
fi
dence interval; RP = radical prostatectomy.
E U R O P E A N U R O L O GY 7 3 ( 2 0 18 ) 3 3
–
3 7
36